 Download Full Guidance
Download Full GuidanceAcute hepatitis C infection is most often asymptomatic and frequently develops into
chronic infection. Case reports of acute hepatitis C in the US increased yearly from 2010
through 2021. Although there was a 6% decrease in acute hepatitis C infections in 2022,
the number of cases in 2022 was still 2 times as high as the number of cases in 2015 (CDC,
2024). Acute HCV infection has most often been associated with parenteral exposures to
blood or body fluids (CDC, 2019). Although HCV infection is primarily associated with
injection drug use (IDU), certain behaviors—for example, unprotected (without a condom)
receptive anal intercourse primarily among men who have sex with men (MSM)—are risk
factors for transmission (Lockart, 2019); (Price, 2019). The syndemic of opioid use disorder and HCV and HIV transmission contributes to the burden of disease in certain populations (Butt, 2020).
Diagnosis of Acute HCV Infection
Recommended Testinga for Diagnosing Acute Hepatitis C Virus Infection |
|
|---|---|
| RECOMMENDED | RATING |
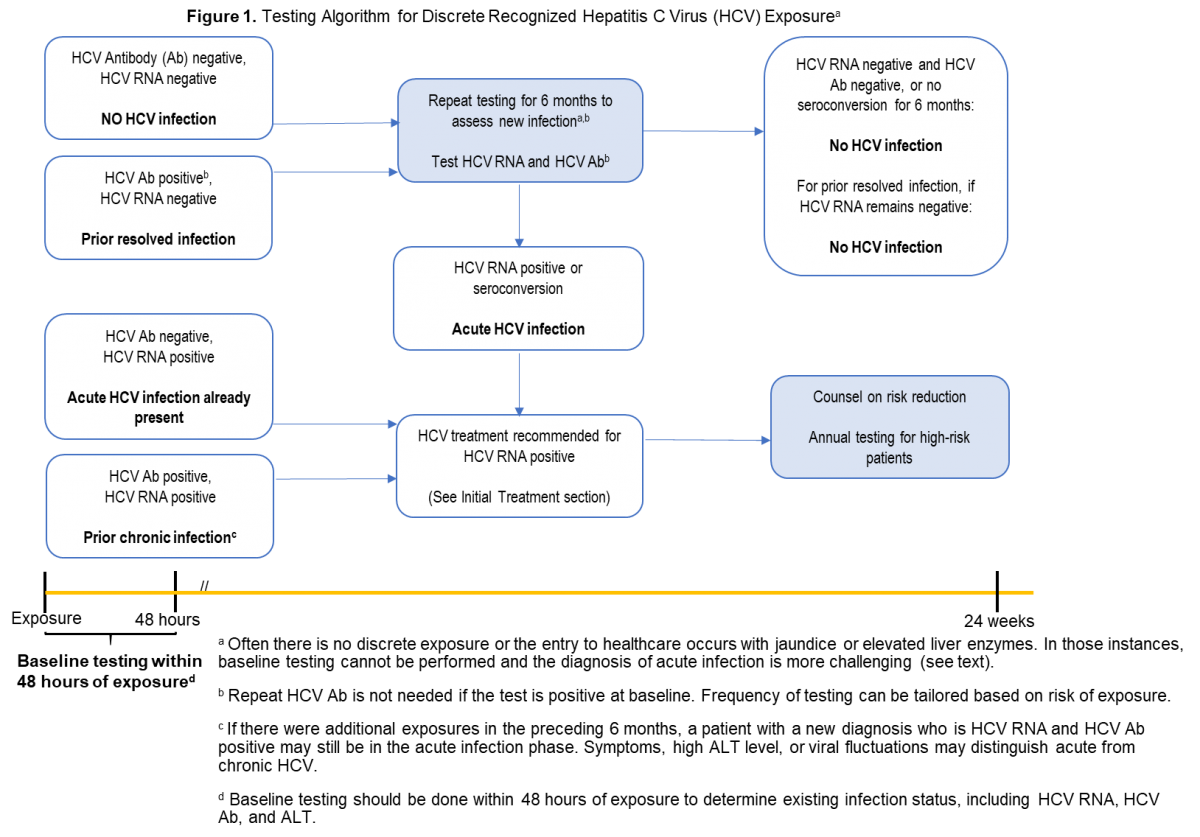
| HCV antibody and HCV RNA testing are recommended when acute hepatitis C infection is suspected due to exposure, clinical presentation, or elevated aminotransferase levels (see Testing Algorithm figure) |
I, C |
| a Recommendations for hepatitis C virus testing are also found in the Testing and Linkage to Care section. |
|
Diagnosis of acute HCV infection enables estimation of annual incidence rates and transmission patterns, thereby facilitating implementation and assessment of prevention programs. At the individual level, a diagnosis of acute infection expedites linkage to care, counseling regarding high-risk behavior, and timely interventions to reduce virus transmission and liver disease progression (Bruneau, 2014). Some persons involved in high-risk behaviors practice serosorting, defined as using HCV antibody serostatus to determine whether to engage in high-risk behaviors with certain individuals (Smith, 2013). Thus, undiagnosed acutely infected persons may be at greater risk of transmitting HCV to their presumably seronegative contacts than would be expected by chance.
The best laboratory evidence to support a diagnosis of acute HCV infection is a positive HCV RNA test in the setting of a negative HCV antibody test (identification during the seronegative window period) (Cox, 2005), or a positive HCV antibody test after a prior negative HCV antibody test (seroconversion). There are rare instances in which these approaches may be misleading, such as in immunosuppressed individuals with impaired antibody production (Chamot, 1990).
Discrete Exposure
The aforementioned types of clear, laboratory-based documentation of acute HCV
infection are most easily achieved when there has been a discrete, known or suspected
exposure (eg, after new onset or a change in drug injection practice, a percutaneous needle
stick exposure to an individual with HCV infection, a potentially nonsterile tattoo, or sexual
assault). In those instances, baseline HCV antibody and HCV RNA testing should be done
within 48 hours of the exposure to document whether there was antecedent HCV infection (see Testing Algorithm figure).
If baseline testing is negative, repeat testing is recommended. Frequency of testing can be tailored based on management objectives (eg, monthly testing to identify and treat acute infection). If baseline HCV antibody testing is positive but HCV RNA testing is negative, repeat HCV RNA and alanine aminotransferase (ALT) testing is recommended to identify an acute reinfection. When baseline HCV antibody and HCV RNA testing are both positive, the person most likely already has chronic HCV infection from prior exposure(s).
No Discrete Exposure
Individuals suspected of having acute HCV infection often do not have a discrete exposure or have no prior baseline testing, making a diagnosis of acute infection more difficult (see Blood Test Interpretation Table). Acute infection should be suspected if there is a new rise in the ALT level without an alternative cause (Kim, 2013); (Blackard, 2008). Acute infection should also be suspected when there are low (especially <104 IU/mL) or fluctuating (>1 log10 IU/mL) HCV RNA values, or spontaneous clearance. These patterns do not commonly occur outside of the first 6 months after HCV infection (McGovern, 2009). In those with a high index of suspicion for HCV exposure (eg, recently relapsed IDU, other high-risk exposure), an HCV RNA should be repeated, if negative.
Persons suspected of having acute HCV infection should also have a laboratory evaluation to exclude other or coexisting causes of acute hepatitis (eg, hepatitis A virus, hepatitis B virus, hepatitis delta virus if chronically infected with hepatitis B virus, and autoimmune hepatitis) (Kushner, 2015). In persons with sexual acquisition of acute HCV infection, evaluation for concurrent genital ulcerative disease and proctitis is recommended (Todesco, 2019); (Goldenberg, 2017). HIV testing should also be performed.
Table. Interpretation of Blood Tests for Diagnosis of Acute HCV Infection
| Test | Interpretation for Diagnosis of Acute HCV Infection |
|---|---|
| HCV Antibody |
|
| HCV RNA |
|
| ALT |
|
ALT, alanine aminotransferase; CD4, CD4-positive T lymphocytes; HCV, hepatitis C virus;
HIV, human immunodeficiency virus; RNA, ribonucleic acid.
Pharmacologic Prophylaxis
Pharmacologic Prophylaxis Not Recommended |
|
|---|---|
| NOT RECOMMENDED | RATING |
| Pre-exposure or post-exposure prophylaxis with antiviral therapy is not recommended | III, C |
There are no data on the efficacy or cost-effectiveness of antiviral therapy for pre-exposure or post-exposure prophylaxis of HCV infection.
Medical Management and Monitoring of Acute HCV Infection
Recommendations for Medical Management and Monitoring of Acute HCV Infection |
|
|---|---|
| RECOMMENDED | RATING |
| After the initial diagnosis of acute HCV with viremia (defined as quantifiable RNA), HCV treatment should be initiated without awaiting spontaneous resolution | I, B |
| Counseling is recommended for patients with acute HCV infection to avoid hepatotoxic insults, including hepatotoxic drugs (eg, acetaminophen) and alcohol consumption, and to reduce the risk of HCV transmission to others | I, C |
| Referral to an addiction medicine specialist is recommended for patients with acute HCV infection related to substance use | I, B |
People with acute HCV infection should be treated upon initial diagnosis without awaiting spontaneous resolution, using a test-and-treat strategy and according to the simplified approach, if eligible. Real-world data have demonstrated a reduction in HCV viremia prevalence and incidence with unrestricted access to HCV therapy (Boerekamps, 2018). In addition, mathematical modeling suggests that direct-acting antiviral (DAA) treatment scale-up, especially among those at highest risk of transmission, can reduce HCV incidence and prevalence (Martin, 2013); (Martin, 2016). Moreover, delay introduced by waiting for spontaneous clearance may be associated with loss to follow up.
Individuals with acute HCV infection should be counseled to reduce behaviors that could result in virus transmission, such as sharing injection equipment and engaging in high-risk sexual practices. Because the risk of transmission of other bloodborne, sexually transmitted infections (eg, HIV and HBV) is higher in the acute infection phase, some experts counsel persons with acute HCV infection to consider using barrier precautions, even in a stable monogamous relationship (see Testing and Linkage to Care). For individuals with acute HCV infection who have a history of recent IDU, referral to harm reduction services and an addiction medicine specialist is recommended when appropriate (Litwin, 2009); (Strathdee, 2005).
People with acute hepatitis C are often asymptomatic or have nonspecific symptoms (eg, fatigue, anorexia, mild or moderate abdominal pain, low-grade fever, nausea, and/or vomiting) that frequently are not recognized as being associated with acute HCV infection. A small proportion (<25%) of persons with acute HCV infection develop jaundice. People diagnosed with acute HCV infection should initially be monitored with hepatic panels (ALT, aspartate aminotransferase [AST], bilirubin, and international normalized ratio [INR] in the setting of an increasing bilirubin level) at 2-week to 4-week intervals (Blackard, 2008). With treatment, a rapid improvement of hepatic laboratory parameters is expected.
There is no need to alter concomitant medications that are metabolized by hepatic enzymes unless there is concern for developing acute liver failure (eg, increasing bilirubin level and INR). Acetaminophen and alcohol consumption should be avoided during acute HCV infection (Curry, 2018); (Proeschold-Bell, 2012); (Dieperink, 2010).
Hospitalization is rarely indicated unless nausea and vomiting are severe. Although acute
liver failure is exceedingly rare (<1%), it represents a serious and life-threatening
complication of acute HCV infection. Persons with an INR >1.5 and those who exhibit any
signs of acute liver failure (eg, hepatic encephalopathy) should be referred to a liver
transplant center immediately. Use of HCV antiviral regimens in acute liver failure should
be managed by a clinician experienced in HCV treatment, ideally in consultation with a liver
transplant specialist.
HCV infection spontaneously clears in 20% to 50% of people (Grebely, 2014) (Kamal, 2008). Clearance of acute HCV infection occurs within 6 months of the estimated time of
infection (median, 16.5 weeks) in at least two-thirds of persons who spontaneously clear
HCV infection. Only 11% of those who remain viremic at 6 months will spontaneously clear
the infection at a later time (Grebely, 2014). People who have spontaneously cleared HCV
infection should not be treated with antiviral therapy. However, they should be counseled
about the possibility of reinfection and tested routinely for this development if risk
behaviors are ongoing (see Testing and Linkage to Care). Of note, transient suppression of viremia can occur in those with acute HCV infection, even among those who progress to chronic infection. Thus, a single undetectable HCV RNA test result is insufficient to declare spontaneous clearance (see Testing and Linkage to Care) (Mosley, 2008); (Villano, 1999).
Predictors of spontaneous clearance include jaundice, elevated ALT level, hepatitis B virus surface antigen (HBsAg) positivity, female sex, younger age, genotype 1 infection, and host genetic polymorphisms, most notably those near the IL28B gene (Kamal, 2008); (Mosley, 2008).
Antiviral Therapy
Recommended Regimens for Persons With Acute HCV Infection |
|
|---|---|
| RECOMMENDED | RATING |
| Owing to high efficacy and safety, the same regimens that are recommended for chronic HCV infection are recommended for acute infection | IIa, C |
A number of studies have evaluated DAA treatment of acute HCV infection. Small single
arm, uncontrolled studies have evaluated 6 weeks or 8 weeks of ledipasvir/sofosbuvir. One
such study demonstrated a 100% SVR rate with 8 weeks of ledipasvir/sofosbuvir among 27
men with acute HCV infection and HIV coinfection (Naggie, 2019). Investigators conducting
another study evaluated 6 weeks of ledipasvir/sofosbuvir in a similar cohort (25/26 with HIV
coinfection). Among participants with genotype 1 infection, 79% (15/19) achieved SVR12;
71% (5/7) of those with genotype 4 infection attained SVR12 with this shortened regimen.
Among the 6 individuals whose treatment did not lead to SVR12, there were 3 relapses; all
had baseline HCV RNA levels >7 log10 IU/mL. Three participants achieved SVR4 but were
lost to follow-up (Rockstroh, 2017b). A phase 2 study evaluating 6 weeks of
ledipasvir/sofosbuvir among 20 individuals with genotype 1 HCV monoinfection, all of
whom attained SVR12 (Deterding, 2017).
An open-label, single-arm, multicenter pilot study evaluated the eAicacy of 6 weeks of the
pangenotypic regimen glecaprevir/pibrentasvir among persons with acute/recent HCV
infection (ie, duration of infection <12 months). SVR12 rate was 90% (27/30); a single
virological failure occurred in a person with genotype 1a infection, HIV coinfection, and a
viral load of 7.7 log10 IU/mL. This individual was successfully retreated (Martinello, 2020).
Another open-label, single-arm, multicenter trial evaluated the eAicacy of 4 weeks of daily
glecaprevir/pibrentasvir among 23 adults with recent HCV infection (duration of infection
<12 months or antibody seroconversion within 18 months). Ninety-six percent of the study
population were men; 70% had HIV coinfection and 74% had genotype 1a infection. SVR12
was attained by 78% (18/23) of participants. Notably, the SVR12 rate among those with
baseline HCV RNA ≤6 log10 was 100% (12/12). No serious adverse events were reported.
Four participants relapsed; 3 were retreated. Two retreated participants attained SVR12
and the third was lost to follow-up (Martinello, 2023). Although the majority of participants
in these small studies evaluating abbreviated courses of glecaprevir/pibrentasvir attained
SVR, the SVR rates were lower than those seen with the longer recommended duration of
treatment (≥8 weeks).
In the only randomized trial to date, investigators compared 6 weeks versus 12 weeks of
sofosbuvir/velpatasvir in the international REACT trial of acute/recent HCV infection. The
study was stopped early due to inferiority of the shortened duration of therapy arm (ie, 6
weeks). In the 6-week arm, SVR rates in the intention-to-treat and modified intention-to
treat analyses were 81.7% (76/93) and 89.4% (76/85), respectively. There were 6 relapses
and 8 nonvirologic failures in the 6-week study arm. In the 12-week study group, SVR rates
in the intention-to-treat and modified intention-to-treat analyses were 90.5% (86/95) and
97.7% (86/88) with no virologic failures. Three participants were lost to follow-up. There
were no clear predictors of relapse aside from shorter treatment duration (Matthews, 2021).
To date, there are insufficient data to support a particular regimen or treatment duration outside of a clinical trial. Until more definitive data are available, treatment as described for chronic hepatitis C is recommended (see Initial Treatment of HCV Infection) for persons with acute HCV infection. Pangenotypic regimens are recommended if HCV genotyping is unavailable or if concern of exposure to more than 1 genotype exists. Using the same regimens to treat acute/recent HCV as for chronic HCV infection also simplifies management, as defining acute HCV infection may be clinically challenging.